If you missed this, keep reading to learn the latest research about these vision-threatening conditions.
“I tried to tell them. I couldn’t see well out of that eye even with new glasses and the doctor said I just had astigmatism. Then it got worse and started in the other eye. I didn’t know how to describe it so they would understand, but it was starting to look like this!”

“I just didn’t feel comfortable driving. “
“Every time I saw the eye doctor, I said it got worse and the doctor agreed. When I asked what to do about it, the doctor replied, ‘We’ll watch it’. The next visit went the same, and I started to think they were going to ‘watch’ me go blind”
This is the sort of story we have been hearing for decades. It’s the story of keratoconus patients worldwide. Once considered a rare disease, keratoconus [ker’-at-o-ko-nus] is now known to affect millions of Americans.
THE PROBLEM:
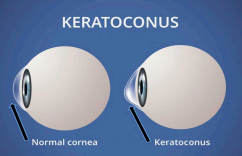
In keratoconus, the clear cornea in the front of the eye bulges forward, becoming thinner and more cone-shaped, distorting your vision even with glasses. This creates not standard astigmatism but irregular astigmatism, which usually cannot be corrected with glasses.
People with keratoconus have a condition that causes them to lose their sight. Patients naturally worry and have questions. There is so much outdated information and misconceptions on the Internet and in textbooks, that making the best and safest choice for your own eyes can bevery confusing. No one wants to make a bad decision.

How much of what you’ve heard or read
about keratoconus and CXL is outdated?
To find out, take these two quick 5 question quizzes.
Did your doctor tell you that your only option is a corneal transplant or scraping off the corneal surface? Learn about major new advancements in treatment options.
TREATMENTS:
In 2001, the original form of a procedure called cross-linking (CXL) was first described. Using vitamin B (riboflavin) and UV light, CXL strengthened the cornea and stopped or slowed progression of the disease. Unable to get the vitamin into the cornea without scraping off the front layer (the epithelium), this protective layer was surgically scraped away or removed with an electric brush before riboflavin drops were applied in the Dresden Procedure. This is why these older procedures are called “Epi-Off.”
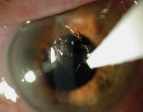

Removal of the eye’s protective epithelium makes the eye susceptible to infection, scarring, melting of the cornea, development of a hole in the front of the eye and more.

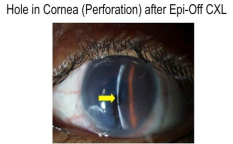
Re:Vision NO LONGER PERFORMS this older, invasive “Epi-Off” procedure.
ADVANCED TREATMENTS:
As the first surgeon to perform the original Epi-Off CXL in the Washington DC area in 2009, Dr. Rubinfeld saw first-hand the pain, slow recovery, and risks of this invasive surgical approach. To better treat his patients, he formed and led the world’s largest keratoconus research study group- CXLUSA.com. By 2012, he and his team had developed effective CXL without corneal scraping described in medical journals and textbooks and The National Keratoconus Foundation. Dr. Rubinfeld has lectured internationally on his unique innovations.

Instead of pain for a week or more (often requiring opioids), months of vision recovery and serious risks; these advances in treatment, which came to be called EpiSmart, allow patients to return to work or school the next day. In this study of 592 eyes, no patients lost vision or had progression of their keratoconus. These results were confirmed In a larger FDA study of 2,228 subjects.
RECOVERY:
Patients who have had EpiSmart Epithelium On crosslinking return to work, school, and normal activities the next day. Because the epithelium is not scraped off, there is no need to wait for the epithelium to grow back and heal and both eyes can be treated on the same day. Patients can travel, exercise and get on with their lives very quickly. The original Epithelium-Off CXL usually requires one or more weeks of recovery and strong pain medication for each eye- which need to be treated individually due to the higher risks and three months apart.
This report describes treatments that are not FDA-approved
WHICH TREATMENT IS BEST FOR YOUR EYES?
- The best possible treatment is when keratoconus is caught early and treated with the best CXL treatment available to prevent any vision loss by stopping progression of the disease. However, because special scanning devices can be needed to detect early keratoconus, all too often the disease is diagnosed when vision has already been lost.
- For patients with more advanced disease who have already lost vision from keratoconus, the use of an FDA-cleared corneal reshaping technology called CK (Conductive Keratoplasty) in combination with our unique CXL has been shown to restore some of their lost vision. This CK device, in use since 2001 worldwide with an excellent safety record, uses radio waves to reshape the cornea without any cutting.

CK (Conductive Keratoplasty) radio pulses reshape corneas
In more advanced keratoconus, the goal is to flatten the elevated “cone” that interferes with vision. CK is performed first to flatten the cone and the next day, CXL is used to strengthen the cornea and make the effect last. In our studies our patients gain several lines of vision and patients we treated with this approach in 2012 have remained stable and better able to see to this day.
GENERAL GUIDELINES:
- For patients caught early who still have good vision with glasses, our advanced CXL is the best option allowing them to return to work or school the next day and preventing future vision loss from keratoconus. No CK is needed.
- For patients with more advanced keratoconus who have lost substantial vision in at least one eye, we have found that CK reshaping followed by CXL has helped them better tolerate glasses or contacts and avoid risky corneal transplants. Vision after CK and CXL is usually improved with a new glasses prescription roughly 3 months after the procedure. Until then, vision normally goes up and down during this healing process, so we usually wait to prescribe new glasses until then. Most patients can wear their contacts about 2-3 days after treatment.
EXPECTATIONS:
CXL or CK combined with CXL is NOT LASIK or cataract surgery. Its objective is not to eliminate glasses and provide “perfect” vision but to stop progressive loss of vision and, in some cases, improve some of the vision lost in more advanced cases.

Dr. Rubinfeld is personally available for complementary consultations to evaluate patients and discuss the best options to diagnose and treat this vision- threatening condition, and answer questions. Please fill out a request form by clicking here or call us at 301-908-8091 to be scheduled.
This report describes treatments that are not FDA-approved