Most of what our patients find on Keratoconus is outdated. To help those with keratoconus and similar conditions, we Googled the most common questions asked. Here are some of them with updated answers, new references and research:

1. “How quickly does keratoconus progress?
It used to be thought that progressive vision loss from keratoconus could be predicted. New research and experience with patients have taught us that this is wrong. People can have stable vision for years and then rapidly and unpredictably lose sight over weeks. This can stop and then another fast drop in vision can occur. This is why eye specialists urge patients to get tested and stop their disease as soon as possible. Without treatment, keratoconus only gets unpredictably worse and not better.
2. At what age does keratoconus stop?
This is another common myth; it doesn’t. We have seen hundreds of patients who were told that their vision loss from keratoconus would stop at the age of 20, 30, 40, 50 or later. We’ve seen patients lose vision rapidly in their 60s from keratoconus. Needless to say, these patients are often frightened, confused and frustrated. Some are angry at the doctors who told them that keratoconus stops at certain ages as they had been taught years ago.

3. I’ve read that Epithelium-On CXL doesn’t work.
Dozens of Epithelium-On CXL systems have been found to NOT WORK effectively in extensive analysis of over 1000 published papers and reviews. In the world’s scientific medical literature; only one Epithelium-On protocol, EpiSmart®, invented by Dr. Rubinfeld, has been shown in large clinical trials to work in stopping KCN worsening and improving vision. This unique, patented investigational system, dubbed EpiSmart®, has been extensively studied in labs and clinical trials for many years.
One reason that EpiSmart® has been shown to work and no other Epithelium-On CXL has, is that no other system has been shown to get the right concentration of vitamin B2 into the cornea. Here is the way we know and can prove this:
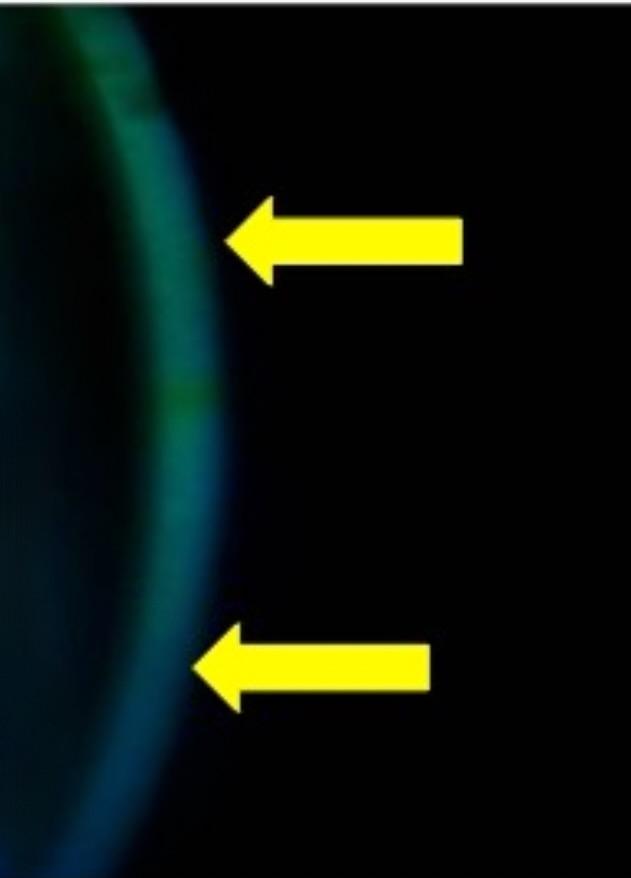
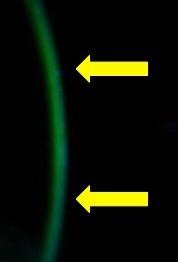
Vitamin B glows green under blue light. On the left, the arrows point out the cornea under blue light after 20 minutes of loading with another Epithelium-On formulation This mild green color is inadequate for effective CXL. On the right the arrows show well loaded, bright green in the cornea after only 10 minutes of loading using the EpiSmart® patented formulation.
Other “Epithelium-On” crosslinking – Inadequate Riboflavin in Cornea
EpiSmart® Epithelium-On crosslinking – Adequate Riboflavin in Cornea
4. How long can I wait to treat my keratoconus?
With a disease that causes unpredictable and often rapid loss of vision, the best answer is really “as soon as you can”. We’ve seen too many patients we had told to be treated who did not. Months and sometimes years later they come back unable to drive or work because of vision loss. In addition to the risk of rapid vision loss without early treatment patients risk a condition called hydrops in which the cornea suddenly and unpredictably becomes painfully swollen as a layer of the cornea bursts.
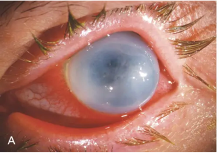
Hydrops Occurs Suddenly in Keratoconus
5. Can you have keratoconus in only one eye?
It may seem so, but keratoconus is defined as a corneal disease that is bilateral (both eyes), asymmetrical (one eye worse than the other) and progressive (it gets worse). The basic corneal weakness that allows the cornea to bulge forward is in both eyes. Patients often ask to only have their “bad eye” treated. Usually, these patients have been relying on their “good eye” to drive, read and function.
The danger with treating only the “bad eye” is that the “good eye” is at risk of suddenly and unpredictably losing vision without warning.
6. Can LASIK fix keratoconus?
Although LASIK can make people with normal corneas see much better, LASIK cannot be used to treat keratoconus. In fact, it will further weaken the cornea and make the keratoconus worse.
7. What should you avoid if you have keratoconus?
Vigorous eye rubbing can weaken the collagen in your cornea which has a major role in keeping the corneal shape round. Much like the collagen in your knees, repeated pressure and injuries will stretch out the collagen and cause problems. Many of our patients have found an over the counter eyedrop called Pataday to reduce eye itch.
8. Why not just replace your cornea with a cornea transplant?
Corneal transplants are very invasive procedures with serious risks including graft rejection of the graft, susceptibility to minor trauma and often a year of recovery and suture removal.
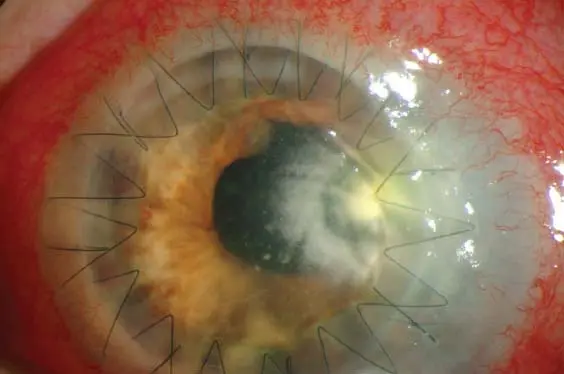
Infected transplant suture
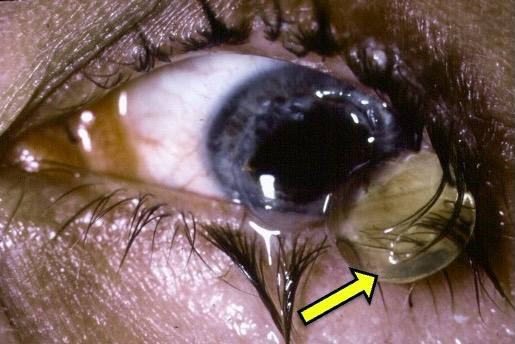
Minor trauma burst this eye years after a transplant.
(Yellow arrow points to natural lens now outside the eye.)
9. Why can’t we just get glasses for keratoconus?
In keratoconus, the cornea becomes irregular in shape, and this can’t be fixed with glasses. Rigid contact lenses can improve vision for keratoconus patients because they flatten down the cornea and deal with some of the irregularity if expertly fitted.
10. If rigid contacts help me see with keratoconus, why can’t I just keep using them?
Rigid contact lenses can help keratoconus patients see better but will NOT STOP PRGRESSIVE VISION LOSS. As keratoconus progresses, you can lose more vision until the contacts won’t work anymore. Also, treatment that allows you to see better with glasses gives your eyes a break from contacts allowing improving the health of your eyes. Contacts can cause serious infections if overworn and this is especially true in keratoconus patients.
11. Does keratoconus run in families?
Yes. If relatives have keratoconus, your chances of having it are increased. This does not mean you will develop it. It does mean that family members should be tested.
12. Why did my other eye doctors not know I had keratoconus?
Diagnosing Keratoconus can involve very expensive scanning technology which most eye doctors don’t have. Also, until recently, keratoconus was thought to be a rare disease so many eye doctors would not suspect it.
13. Will Crosslinking eliminate the need for glasses or contacts?
Crosslinking is designed to stop the progressive vision loss due to keratoconus. It is very different from LASIK or cataract surgery, so most patients still need glasses or contacts after treatment of their keratoconus.
14. When can I return to my normal activities?
Most patients who have the proprietary Epithelium-On crosslinking procedure return to work or school the next day. Because the epithelium is not surgically removed, there is no need to wait until the epithelium grows back and heals so patients can travel, exercise and get on with their lives very quickly.
15. I’ve heard of Intacs for keratoconus. What are they?
Intacs are plastic implants that have been used to try and improve vision in patients with keratoconus. They do not stop vision loss from keratoconus and there can be issues where these plastic implants need to be removed.
16. What if I waited and already lost vision from Keratoconus? Is there a way to restore some of the lost vision?
Although each patient is different, we have had excellent results doing this by first reshaping the cornea non-invasively with radio waves to flatten the big bumps in the cornea and then “locking in” the effect and preventing further vision loss using our proprietary epithelium-on CXL. These results have been seen to last for a long time. In our practice, we have seen patients 14 years after our treatment who retain their improved vision and don’t lose any more vision.
17. How often do patients need retreatments?
Simply put, very rarely. We have seen many patients that we treated with these techniques since 2012, and they are remarkably stable. This is consistent with our published research showing EpiSmart® treatments to be more effective than Epi-Off treatments.
In fact, we find that we’ve had to retreat patients who had Epi-Off CXL; as the literature describes that this treatment fails 8% of the time and the EpiSmart® treatment has proven to be more effective.
In this publication, a patient had Epi-Off CXL and complications. We performed an EpiSmart® type treatment which succeeded and avoided complications.
These are just a few of the questions patients ask. Please ask us any others that come to mind.

Dr. Rubinfeld is personally available for complementary consultations to evaluate patients and discuss the best options to diagnose and treat this vision- threatening condition, and answer questions. Please fill out a request form by clicking here or call us at 301-908-8091 to be scheduled.
To read the latest published research for yourself, see cxlusa.com